
Clinical Protocol: Optimizing the 12-Week ICBC Active Rehabilitation Framework Through Multi-Disciplinary Allied Healthcare

Figure 1: Physiotherapy intervention targeting persistent neurodynamic tension. Within our 12-week ICBC structure, our physiotherapists facilitate early motor desensitization and local stabilizer activation—essential steps for transitioning patients from acute pain to the whole-body functional loading required for a safe return to work across the Fraser Valley.
Motor vehicle accidents (MVAs) within the Fraser Valley frequently result in complex acceleration-deceleration injuries, including cervical acceleration-deceleration (CAD) syndromes, multi-level spinal segmental dysfunction, and neurodynamic tension. Near Me Therapy delivers an integrated, evidence-informed 12-week ICBC active rehabilitation program designed to restore arthro-kinematic mobility, downregulate central nervous system hypersensitivity, and rebuild neuromuscular capacity. Utilizing pre-approved ICBC kinesiology funding alongside collaborative Physiotherapy, Chiropractic Care, Registered Massage Therapy (RMT), and Acupuncture, our clinical team targets soft-tissue scarring, peripheral nerve entrapments, and aberrant movement adaptations. While primary uncomplicated soft-tissue pathomechanics target a standard 12-week functional discharge, our framework integrates clinical variability pathways to accommodate chronic pain syndromes, multi-site comorbidity profiles, and complex tissue healing timelines. This synchronized care model addresses the unique postural stressors of commuting professionals and industrial laborers across the Township of Langley, Langley City, and East Surrey, providing direct access to structured, objective recovery pathways that facilitate a safe, durable return to pre-accident functional status.
The Science of it and Clinical Presentation
The physical impact of a motor vehicle accident extends far beyond superficial bumps and bruises. During a rear-end or side-impact collision—events that occur daily along busy local routes like the Highway 1 corridor, 200th Street, and Fraser Highway—the human spine is subjected to sudden, violent forces. This rapid shifting whips the neck and back through an unnatural S-shaped curve, stretching and micro-tearing the stabilizing ligaments, spraining the small joints of the spine, and severely straining the surrounding muscles.
Patients who experience these crash dynamics encounter very specific structural changes in their bodies. On a muscular level, the body tries to protect itself by locking up. Muscles like the trapezius, levator scapulae, and the deep stabilizers of the lower back go into a state of constant, painful contraction. If you look closely at these tissues, you will find tight, highly sensitive knots known as myofascial trigger points. Because these tight bands are locked down, local blood flow is restricted. This deprives the muscle tissue of oxygen, causes metabolic waste to pool, and fires off deep pain signals to the brain.
When nearby nerves are compressed or pinched by swollen muscles and inflamed tissues, the patient begins to feel neurological symptoms. This presents as radiating arm or leg pain, burning sensations, tingling, or numbness that travels along specific nerve pathways. Left unmanaged, the body replaces this initial swelling with dense, disorganized scar tissue. This stiff fibrous tissue acts like internal glue, binding different layers of muscle and fascia together, which permanently restricts normal movement and forces the patient into unnatural, guarded postures.
These physical issues are made worse by the daily routines of people living and working in the Fraser Valley. For example, a project manager who regularly commutes from Willoughby or Walnut Grove over the Golden Ears Bridge spends hours sitting in a car. This sustained sitting places a heavy, unmoving load on a damaged lower back, aggravating disc pressure and deep hip tightness. On the other hand, tradespeople and manual workers living in areas like Cloverdale or Brookswood often reinjure healing tissues by lifting heavy loads at work, forcing their bodies to use compensating muscles that quickly become exhausted and painful.
Clinical Variability: Modifying Care for Complex and Chronic Pain
While a standard, straightforward soft-tissue injury can successfully progress toward a 12-week discharge, clinical experience shows that recovery from trauma is rarely identical for everyone. For patients who already have degenerative disc changes, arthritis, or existing health conditions like diabetes, the recovery timeline changes. In these complicated cases, the central nervous system can enter a state of high alert. When this happens, the spinal cord amplifies pain signals, causing the brain to interpret normal, gentle movements or light pressure as severe physical threats.
If a patient is dealing with this type of hypersensitive nervous system or a baseline of chronic pain, rushing them into aggressive exercises or intense adjustments can backfire, causing severe symptom flare-ups that stall progress. Because of this, our 12-week protocol is designed to be highly flexible. It serves as a structural guide that can be adapted to slow down exercise progressions, extend hands-on therapies, or request treatment extensions from ICBC when objective functional goals require more time.
The Integrated Multi-Disciplinary Intervention
Isolating a patient to just one type of therapy often fails to address the multi-layered damage caused by an automobile accident. Near Me Therapy utilizes a structured, team-based care pathway where different health professionals focus on different layers of the same injury at the exact same time.
Phase 1: Joint and Nerve Modulation (Weeks 1–4)
The first few weeks after an ICBC accident focus entirely on calming down a hyper-reactive nervous system, restoring basic joint movement, and relieving intense nerve irritation.
Chiropractic Care: Focuses directly on spinal joints that have become locked up or restricted due to the force of the collision. By performing gentle joint mobilizations or precise adjustments, the chiropractor restores normal spinal alignment, reduces joint stiffness, and stimulates internal nerve receptors that help block pain signals from reaching the brain. For highly sensitive or chronic pain patients, manual adjustments are swapped for gentle instrument-assisted techniques to avoid over-stimulating the nervous system.
Physiotherapy: Functions as an immediate triage step to manage nerve irritation. The physiotherapist checks for nerve tension and introduces gentle neural gliding techniques to reduce swelling around nerve roots. To help wake up muscles that have shut down from pain, they may use Intramuscular Stimulation (IMS) or dry needling. This involves using thin needles to reach deep, tight knots, forcing the muscle to twitch, relax, reset, and receive fresh blood flow.
Acupuncture: Works alongside joint and nerve treatments to manage overall pain. By placing sterile needles into specific neurofunctional points, the acupuncturist helps calm down a stressed nervous system and prompts the brain to release its own natural pain-relieving chemicals, reducing the body's urge to lock up in pain.
Phase 2: Tissue Realignment and Soft-Tissue Loading (Weeks 5–8)
Once acute joint restrictions and severe nerve pain have settled, treatment shifts to modifying the physical structure of the muscles and fascia so the patient can start moving comfortably.
Registered Massage Therapy (RMT): Targets the dense, disorganized scar tissue and tight fascial layers caused by the accident. The RMT uses specialized myofascial release, deep tissue friction, and neuromuscular massage to stretch out restricted fascial planes and help realign scar tissue fibers. This hands-on work makes the muscles more pliable, restores their normal resting length, and improves fluid drainage to bring fresh nutrients to healing areas.
Functional Chiropractic Care: For chiropractors who focus heavily on soft-tissue therapies, Phase 2 shifts from basic joint alignment to active soft-tissue work under tension. Using techniques like Active Release Techniques (ART) or instrument-assisted scraping, the chiropractor holds a tight muscle in place while the patient actively moves through a comfortable range of motion. This breaks down stubborn friction between deep muscle layers, improves tissue length under safe conditions, and prepares the muscle to handle real-world physical stress.
Physiotherapy Integration: During this phase, the physiotherapist builds upon the improved muscle flexibility achieved through massage and active chiropractic work. They use manual joint glides to improve deep movement and introduce early coordination drills, ensuring the brain learns how to safely control and balance these newly recovered ranges of motion.
Phase 3: Muscle Stabilization and Advanced Loading (Weeks 9–12+)
The final phase of recovery moves away from hands-on, passive care and shifts toward independent physical strengthening, ensuring the body can handle daily life without reinjury.
Kinesiology / Active Rehabilitation: Utilizing pre-approved ICBC Kinesiology sessions, the kinesiologist transitions the patient into a structured exercise program. Working from the initial assessments provided by the physiotherapist and chiropractor, the kinesiologist designs a personalized workout routine targeting the deep core stabilizers of the neck and lower back. This phase focuses on correcting poor movement habits, rebuilding core stability, and improving muscle endurance so the body can handle driving through Langley or returning to manual labor in Surrey.
Coordinated Team Support: Rather than stopping treatment abruptly, the chiropractor and physiotherapist stay involved during this high-load phase. The chiropractor monitors how the spine behaves under resistance, adjusting joint structures as the physical demands increase. At the same time, the physiotherapist performs advanced functional movement tests, checks how the nerves respond to fatigue, and uses targeted IMS treatment if any secondary stabilizer muscles begin to tighten up or overwork as the exercises progress.
Coordinated Care Pathway Map
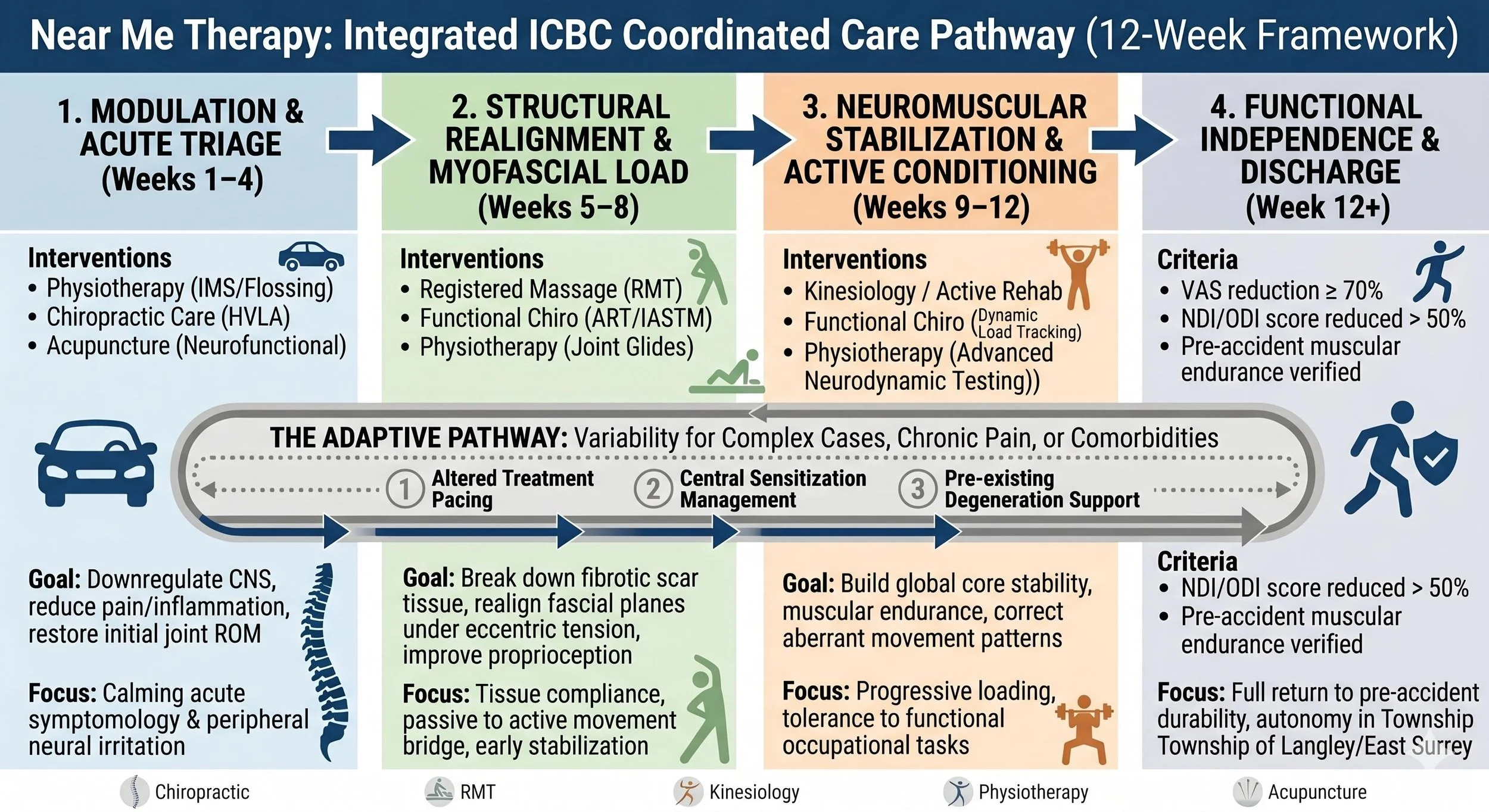
Figure 2:Near Me Therapy’s multi-disciplinary ICBC recovery framework. This clinical roadmap illustrates the step-by-step transition from acute joint and nerve desensitization to active kinesiology loading. The built-in "Adaptive Pathway" loop highlights how our Langley and Surrey clinical teams modify exercise pacing and hands-on therapy timelines to accommodate complex comorbidities, pre-existing degenerative conditions, and centralized chronic pain.
Objective Progression Metrics and Adaptive Benchmarks

Figure 3: Near Me Therapy’s data matrix separating standard recovery milestones from our adaptive clinical loops. While uncomplicated soft-tissue cases systematically progress toward functional discharge by Week 12 using clear physical benchmarks, patients experiencing central nervous system hypersensitivity, prior structural trauma, or multi-site comorbidities are seamlessly transitioned into custom pacing, tissue desensitization protocols, and comprehensive ICBC case extension tracking.
To systematically evaluate injury recovery following a motor vehicle accident, Near Me Therapy utilizes a dual-layered benchmark tracking system that contrasts standard recovery timelines with adaptive clinical variance pathways. For straightforward soft-tissue presentations, recovery is gauged against clear, objective metrics across a 12-week horizon: achieving a 30% reduction in the Visual Analog Scale (VAS) and a 20% improvement in spinal range of motion by Week 4; establishing pain-free nerve tracking and a 20% reduction in disability indexes by Week 8; and confirming that muscular endurance matches pre-accident baselines within 15% during a 45-minute supervised kinesiology session by Week 12. However, for complex or chronic cases—such as patients experiencing central sensitization, pre-existing joint degeneration, or systemic comorbidities—the framework automatically pivots to an Adaptive Care Pathway Loop. This diversion slows treatment pacing, shifts high-velocity adjustments to gentle activator or drop-table mobilizations, and swaps deep myofascial shearing for soothing parasympathetic techniques. Rather than forcing a hypersensitive nervous system to meet rigid time constraints, our team uses these clinical deviations to regulate autonomic tone, deliver patient pacing education, and generate detailed functional reports to secure necessary ICBC treatment extensions, ensuring a safe and lasting return to occupational durability.
Evidence-Informed Clinical References
Whiplash and Spine Biomechanics:Spine Journal - Biomechanical Analyses of Whiplash Impact Dynamics
Nerve Mobilization Techniques:Journal of Orthopaedic & Sports Physical Therapy - Clinical Applications of Neurodynamic Techniques
Nervous System Hypersensitivity:The Journal of Pain - Mechanisms and Management of Chronic Pain and Central Sensitization
Whiplash Recovery Guidelines:BC Medical Journal - Evidence-Based Management of Whiplash-Associated Disorders
ICBC Claims and Provider Regulations:ICBC Health Services Strategy and Allied Health Provider Guides